
Our Health Library information does not replace the advice of a doctor. Please be advised that this information is made available to assist our patients to learn more about their health. Our providers may not see and/or treat all topics found herein.
Anal Cancer Treatment (PDQ®): Treatment - Patient Information [NCI]
General Information About Anal Cancer
Anal cancer is a type of cancer that forms in the tissues of the anus.
The anus is the end of the large intestine. It is where stool (solid waste) leaves the body. The anus is formed partly from the outer skin layers of the body and partly from the intestine. The anus is connected to the rectum by the anal canal, which is about 1 to 1½ inches long. This area is controlled by two ring-like sphincter muscles, which contract to hold stool in and relax to allow its passage out of the body. 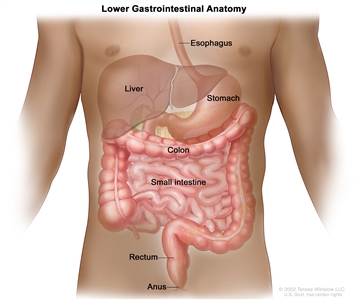
Anatomy of the lower gastrointestinal (digestive) system showing the colon, rectum, and anus. Other organs that make up the digestive system are also shown.
Anal cancer can start in the lining of the anal canal, called the mucosa, or in the perianal skin, the squamous cells outside of the anus that contain hair follicles and sweat glands.
Tumors of the perianal skin that do not involve the anal sphincter are usually treated the same as anal cancers, although local therapy (treatment directed to a limited area of skin) may be used for some.
Most anal cancers are related to human papillomavirus (HPV) infection.
Anal cancer is caused by certain changes to the way anal cells function, especially how they grow and divide into new cells. There are many risk factors for anal cancer, but many do not directly cause cancer. Instead, they increase the chance of DNA damage in cells that may lead to anal cancer. Learn more about how cancer develops at What Is Cancer?
A risk factor is anything that increases the chance of getting a disease. Some risk factors for anal cancer can be changed. However, risk factors also include things people cannot change, like getting older and their health history. Learning about risk factors for anal cancer can help you make changes that might lower your risk of getting it.
Risk factors for anal cancer include:
- being infected with a high-risk human papillomavirus (HPV), especially HPV type 16 or 18. Learn more about HPV and Cancer.
- having a condition or disease that causes a weakened immune system, such as HIV or an organ transplant
- having a personal history of vulvar, vaginal, or cervical cancers
- having many sexual partners
- having receptive anal intercourse (anal sex)
- smoking cigarettes. Learn more about Tobacco (includes help with quitting).
Talk with your doctor if you think you may be at risk.
Signs of anal cancer include bleeding from the anus or rectum or a lump near the anus.
These and other signs and symptoms may be caused by anal cancer or by other conditions. Check with your doctor if you have:
- bleeding from the anus or rectum
- a lump near the anus
- pain or pressure in the area around the anus
- itching or discharge from the anus
- a change in bowel habits
Tests that examine the rectum and anus are used to diagnose anal cancer.
In addition to asking about your personal and family health history and doing a physical exam, your doctor may perform the following tests and procedures:
- Digital rectal examination (DRE) is an exam of the anus and rectum. The doctor or nurse inserts a lubricated, gloved finger into the lower part of the rectum to feel for lumps or anything else that seems unusual.
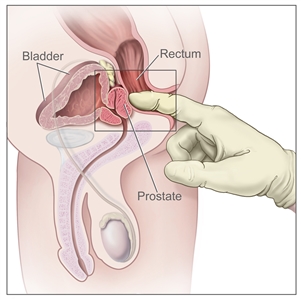
Digital rectal exam (DRE). The doctor inserts a gloved, lubricated finger into the rectum and feels the rectum, anus, and prostate (in males) to check for anything abnormal. - Anoscopy is an exam of the anus and lower rectum using a short, lighted tube called an anoscope.
- Proctoscopy is a procedure to look inside the rectum and anus to check for abnormal areas, using a proctoscope. A proctoscope is a thin, tube-like instrument with a light and a lens for viewing the inside of the rectum and anus. It may also have a tool to remove tissue samples, which are checked under a microscope for signs of cancer.
- Endo-anal or endorectal ultrasound is a procedure in which an ultrasound transducer (probe) is inserted into the anus or rectum and used to bounce high-energy sound waves (ultrasound) off internal tissues or organs and make echoes. The echoes form a picture of body tissues called a sonogram.
- Biopsy is the removal of cells or tissues so they can be viewed under a microscope by a pathologist to check for signs of cancer. If an abnormal area is seen during the anoscopy, a biopsy may be done at that time.
After anal cancer has been diagnosed, tests are done to find out if cancer cells have spread within the anus or to other parts of the body.
The process used to find out if cancer has spread within the anus or to other parts of the body is called staging. The information gathered from this staging process determines the stage of the disease. It is important to know the stage in order to plan treatment. The following tests may be used in the staging process:
- CT scan (CAT scan) uses a computer linked to an x-ray machine to make a series of detailed pictures of areas inside the body, such as the abdomen, pelvis, or chest. The pictures are taken from different angles and are used to create 3-D views of tissues and organs. A dye may be injected into a vein or swallowed to help the organs or tissues show up more clearly. This procedure is also called computed tomography, computerized tomography, or computerized axial tomography.
- Chest x-ray is a type of radiation that can go through the body and make pictures of the organs and bones inside the chest.
- MRI (magnetic resonance imaging) uses a magnet, radio waves, and a computer to make a series of detailed pictures of areas inside the body. This procedure is also called nuclear magnetic resonance imaging (NMRI).
- PET scan (positron emission tomography scan) uses a small amount of radioactive glucose that is injected into a vein. The PET scanner rotates around the body and makes pictures of where glucose is being used in the body. Cancer cells show up brighter in the picture because they are more active and take up more glucose than normal cells do.
- Pelvic exam is an exam of the vagina, cervix, uterus, fallopian tubes, ovaries, and rectum. A speculum is inserted into the vagina and the doctor or nurse looks at the vagina and cervix for signs of disease. A Pap test of the cervix is usually done. The doctor or nurse also inserts one or two lubricated, gloved fingers of one hand into the vagina and places the other hand over the lower abdomen to feel the size, shape, and position of the uterus and ovaries. The doctor or nurse also inserts a lubricated, gloved finger into the rectum to feel for lumps or abnormal areas.
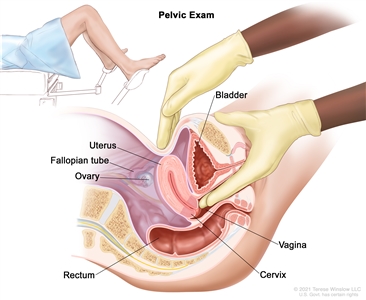
Pelvic exam. A doctor or nurse inserts one or two lubricated, gloved fingers of one hand into the vagina and presses on the lower abdomen with the other hand. This is done to feel the size, shape, and position of the uterus and ovaries. The vagina, cervix, fallopian tubes, and rectum are also checked.
Some people decide to get a second opinion.
You may want to get a second opinion to confirm your anal cancer diagnosis and treatment plan. If you seek a second opinion, you will need to get medical test results and reports from the first doctor to share with the second doctor. The second doctor will review the pathology report, slides, and scans. They may agree with the first doctor, suggest changes or another treatment approach, or provide more information about your cancer.
Learn more about choosing a doctor and getting a second opinion at Finding Cancer Care. You can contact NCI's Cancer Information Service via chat, email, or phone (both in English and Spanish) for help finding a doctor, hospital, or getting a second opinion. For questions you might want to ask at your appointments, visit Questions to Ask Your Doctor About Cancer.
Certain factors affect the prognosis (chance of recovery) and treatment options.
The prognosis depends on:
- the size of the tumor
- whether the cancer has spread to the lymph nodes
The treatment options depend on:
- the stage of the cancer
- where the tumor is in the anus
- whether the person has HIV
- whether cancer remains after initial treatment or has recurred (come back)
Stages of Anal Cancer
Cancer stage describes the extent of cancer in the body, such as the size of the tumor, whether it has spread, and how far it has spread from where it first formed. It is important to know the stage of the anal cancer to plan the best treatment.
There are several staging systems for cancer that describe the extent of the cancer. Anal cancer staging usually uses the TNM staging system. The cancer may be described by this staging system in your pathology report. Based on the TNM results, a stage (I, II, III, or IV, also written as 1, 2, 3, or 4) is assigned to your cancer. When talking to you about your diagnosis, your doctor may describe the cancer as one of these stages.
Learn about tests to stage anal cancer. Learn more about Cancer Staging.
The following stages are used for anal cancer:
Stage 0 (carcinoma in situ)
In stage 0, abnormal cells are found in the mucosa (innermost layer) of the anus. These abnormal cells may become cancer and spread into nearby normal tissue. Stage 0 is also called high-grade intraepithelial lesion (HSIL).
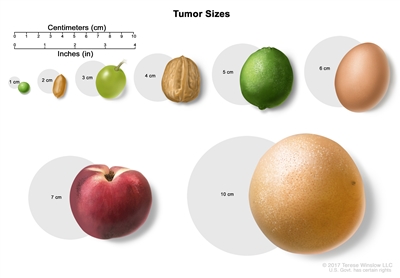
Tumor sizes are often measured in centimeters (cm) or inches. Common food items that can be used to show tumor size in cm include: a pea (1 cm), a peanut (2 cm), a grape (3 cm), a walnut (4 cm), a lime (5 cm or 2 inches), an egg (6 cm), a peach (7 cm), and a grapefruit (10 cm or 4 inches).
Stage I (also called stage 1) anal cancer
In stage I, cancer has formed and the tumor is 2 centimeters or smaller.
Stage II (also called stage 2) anal cancer
Stage II anal cancer is divided into stages IIA and IIB.
- In stage IIA, the tumor is larger than 2 centimeters but not larger than 5 centimeters.
- In stage IIB, the tumor is larger than 5 centimeters.
Stage III (also called stage 3) anal cancer
Stage III anal cancer is divided into stages IIIA, IIIB, and IIIC.
- In stage IIIA, the tumor is 5 centimeters or smaller and has spread to lymph nodes near the anus or groin.
- In stage IIIB, the tumor is any size and has spread to nearby organs, such as the vagina, urethra, or bladder. Cancer has not spread to lymph nodes.
- In stage IIIC, the tumor is any size and may have spread to nearby organs. Cancer has spread to lymph nodes near the anus or groin.
Stage IV (also called stage 4) anal cancer
In stage IV, the tumor is any size. Cancer may have spread to lymph nodes or nearby organs and has spread to other parts of the body, such as the liver or lungs.
Stage IV anal cancer is also called metastatic anal cancer. Metastatic cancer happens when cancer cells travel through the lymphatic system or blood and form tumors in other parts of the body. The metastatic tumor is the same type of cancer as the primary tumor. For example, if anal cancer spreads to the liver, the cancer cells in the liver are actually anal cancer cells. The disease is called metastatic anal cancer, not liver cancer. Learn more in Metastatic Cancer: When Cancer Spreads.
Anal cancer can recur (come back) after it has been treated.
Recurrent anal cancer is cancer that has come back after it has been treated. If anal cancer comes back, it may come back in the anus or in other parts of the body, such as the liver or lungs. Tests will be done to help determine where the cancer has returned. The type of treatment for recurrent anal cancer will depend on where it has come back.
Learn more in Recurrent Cancer: When Cancer Comes Back. Information to help you cope and talk with your health care team can be found in the booklet When Cancer Returns.
Treatment Option Overview
There are different types of treatment for people with anal cancer.
Different types of treatments are available for anal cancer. You and your cancer care team will work together to decide your treatment plan, which may include more than one type of treatment. Many factors will be considered, such as the stage of the cancer, your overall health, and your preferences. Your plan will include information about your cancer, the goals of treatment, your treatment options and the possible side effects, and the expected length of treatment.
Talking with your cancer care team before treatment begins about what to expect will be helpful. You'll want to learn what you need to do before treatment begins, how you'll feel while going through it, and what kind of help you will need. To learn more, visit Questions to Ask Your Doctor About Treatment.
The following types of treatment are used:
Surgery
- Local resection is a surgical procedure in which the tumor is cut from the anus along with some of the healthy tissue around it. Local resection may be used if the cancer is small and has not spread. This procedure may save the sphincter muscles so the person can still control bowel movements. Tumors that form in the lower part of the anus can often be removed with local resection.
- Abdominoperineal resection is a surgical procedure in which the anus, the rectum, and part of the sigmoid colon are removed through an incision made in the abdomen. The doctor sews the end of the intestine to an opening, called a stoma, made in the surface of the abdomen so body waste can be collected in a disposable bag outside of the body. This is called a colostomy. Lymph nodes that contain cancer may also be removed during this operation. This procedure is used only for cancer that remains or comes back after treatment with radiation therapy and chemotherapy.
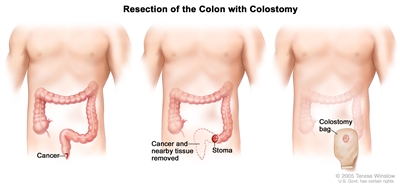
Resection of the colon with colostomy. Part of the colon containing the cancer and nearby healthy tissue are removed, a stoma is created, and a colostomy bag is attached to the stoma.
Radiation therapy
Radiation therapy uses high-energy x-rays or other types of radiation to kill cancer cells or keep them from growing. There are two types of radiation therapy used to treat anal cancer:
- External radiation therapy uses a machine outside the body to send radiation toward the area of the body with cancer.
- Internal radiation therapy uses a radioactive substance sealed in needles, seeds, wires, or catheters that are placed directly into or near the cancer.
Learn more about Radiation Therapy to Treat Cancer and Radiation Therapy Side Effects.
Chemotherapy
Chemotherapy (also called chemo) uses drugs to stop the growth of cancer cells, either by killing the cells or by stopping the cells from dividing. When chemotherapy is taken by mouth or injected into a vein or muscle, the drugs enter the bloodstream and can reach cancer cells throughout the body (systemic chemotherapy).
Chemotherapy drugs used to treat anal cancer include:
- capecitabine
- cisplatin
- fluorouracil
- mitomycin
Combinations of these drugs may be used. Other chemotherapy drugs not listed here may also be used.
Chemotherapy may be combined with other types of treatment, such as radiation therapy.
Learn more about how chemotherapy works, how it is given, common side effects, and more at Chemotherapy to Treat Cancer and Chemotherapy and You: Support for People With Cancer.
New types of treatment are being tested in clinical trials.
For some people, joining a clinical trial may be an option. There are different types of clinical trials for people with cancer. For example, a treatment trial tests new treatments or new ways of using current treatments. Supportive care and palliative care trials look at ways to improve quality of life, especially for those who have side effects from cancer and its treatment.
You can use the clinical trial search to find NCI-supported cancer clinical trials accepting participants. The search allows you to filter trials based on the type of cancer, your age, and where the trials are being done. Clinical trials supported by other organizations can be found on the ClinicalTrials.gov website.
Learn more about clinical trials, including how to find and join one, at Clinical Trials Information for Patients and Caregivers.
Treatment for anal cancer may cause side effects.
For information about side effects caused by treatment for cancer, visit our Side Effects page.
Follow-up care may be needed.
As you go through treatment, you will have follow-up tests or check-ups. Some tests that were done to diagnose or stage the cancer may be repeated to see how well the treatment is working. Decisions about whether to continue, change, or stop treatment may be based on the results of these tests.
Some of the tests will continue to be done from time to time after treatment has ended. The results of these tests can show if your condition has changed or if the cancer has recurred (come back).


This information does not replace the advice of a doctor. Ignite Healthwise, LLC disclaims any warranty or liability for your use of this information. Your use of this information means that you agree to the Terms of Use and Privacy Policy. Learn how we develop our content.
Healthwise, Healthwise for every health decision, and the Healthwise logo are trademarks of Ignite Healthwise, LLC.